Editorial notice: Reviewed for underwriting accuracy by the RJI Underwriting Research Team | Published: June, 2026 | Last reviewed: June, 2026.
————————————————————————————————————–
Executive Summary
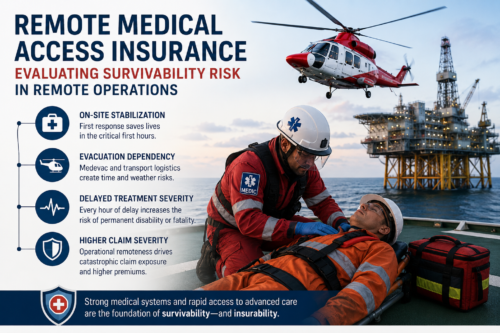
Remote medical access insurance evaluates the realistic probability that an injured worker can be kept alive and stable in an isolated environment before advanced clinical care can be reached. In high-risk, isolated industries, insurers do not just price the likelihood of an accident; they evaluate how delayed stabilization, medevac dependency, and severe operational remoteness can cause survivability to deteriorate. Without robust on-site intervention systems, standard, survivable injuries rapidly escalate into catastrophic permanent disability or fatality claims.
Important Clarification: This article is not about consumer telemedicine services or general remote healthcare access. It explains how insurers evaluate survivability risk in isolated industrial environments where delayed evacuation, limited trauma capability, and operational remoteness can transform survivable injuries into catastrophic insurance claims.
What Is Remote Medical Access in Insurance Underwriting?
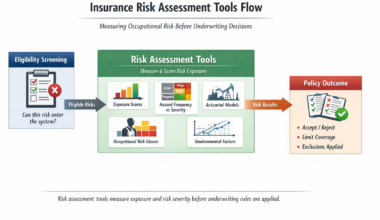
In standard occupational underwriting, risk assessment focuses primarily on injury frequency and baseline workplace safety. However, for isolated job sites, such as deepwater drilling rigs, remote wilderness pipelines, or interior mining operations, insurers must utilize specialized remote medical access insurance frameworks.
This discipline functions fundamentally as survivability-continuity underwriting rather than simple injury-probability underwriting. It does not merely look at whether an incident will occur, but evaluates the entire lifecycle of emergency response through:
-
Stabilization-Probability Underwriting: Assessing the likelihood that the on-site team can keep a worker alive during the critical first hours following a severe trauma.
-
Operational Survivability: The baseline capability of an isolated workplace to prevent an injury from becoming fatal due to its geographic environment.
-
Delayed-Treatment Severity: Actuarial accounting of how fast advanced care becomes reachable. Workers often assume survival depends on the injury itself; insurers know survival depends on the mitigation of treatment-delay severity.
-
Treatment Continuity: The seamless handoff of a patient from on-site first responders to evacuation teams without a drop in life-support quality.
-
Evacuation Dependency: The operational reliance on complex logistical systems, such as long-range helicopters or marine vessels, to move an injured worker to a trauma center.
-
Medical-Response Degradation: The breakdown in life-support efficacy when care is delivered in unstable, isolated, or moving environments.
Underwriters use these factors to judge if an employer’s emergency systems can realistically preserve a worker’s life until advanced treatment becomes accessible. For insurers, remote medical access directly affects occupational coverage pricing, catastrophic injury reserves, disability severity projections, and overall underwriting appetite for isolated operations.
The Mechanics of Operational Remoteness
When an industrial facility is located in a metropolitan area, an emergency call brings a fully equipped advanced life support ambulance within minutes, transferring the patient directly to a nearby Level 1 trauma center. In remote operations, that safety net disappears. Insurers closely scrutinize remote medical access because severe operational remoteness fundamentally shifts the financial severity of any given claim.
Underwriters frequently benchmark remote trauma access against trauma-center capability standards established by the American College of Surgeons. Underwriting severity increases when operational isolation weakens stabilization capability, delays definitive treatment, and increases survivability uncertainty.
When evaluating a risk, underwriters measure the physical distance from major trauma centers and the inevitable delayed emergency response times. Communication limitations, such as satellite drops or dead zones, can stall a rescue launch, while limited on-site treatment capabilities mean that a patient may overwhelm a tiny clinic. These factors lead to delayed specialist access, meaning a complex injury remains unaddressed for twelve, twenty-four, or forty-eight hours.
To account for this, insurers look deep into the mechanics of Offshore Risk Underwriting: How Insurers Evaluate Marine & Remote Workers to determine how these geographical gaps alter the risk profile. If an operator cannot prove their on-site systems can bridge this timeline, insurers face a materially less predictable catastrophic severity profile, resulting in heavily restricted policy terms or significantly higher premiums.
At a certain point, operational isolation moves beyond standard underwriting assumptions and becomes survivability uncertainty. When underwriters cannot confidently model evacuation timelines or treatment continuity, insurer appetite declines sharply, and coverage restrictions become significantly more aggressive.
Golden Hour Degradation & Survival-Window Compression
In emergency medicine, the “Golden Hour” represents the critical window during which rapid trauma stabilization and surgical intervention yield the highest probability of survival and recovery. In remote industrial environments, insurers plan for Golden Hour degradation underwriting because this window is routinely compromised or entirely lost. Trauma survivability timelines are strongly influenced by emergency-response principles published by the National Association of Emergency Medical Technicians.
As treatment windows collapse, injuries worsen rapidly:
-
Internal Bleeding: Without immediate access to a general surgeon, internal hemorrhaging cannot be mechanically stopped. On-site medics can give fluids, but the patient experiences steady decompensation.
-
Crush Injuries: Common in heavy mining and structural ironwork, releasing a trapped limb can flood the body with toxins, causing rapid kidney failure if advanced dialysis and stabilization are unavailable.
-
Severe Burns: Industrial explosions require massive, immediate fluid resuscitation and sterile environment controls to stop progressive shock and catastrophic infection.
-
Neurological Deterioration: Traumatic brain injuries or spinal fractures require immediate intracranial pressure management or surgical alignment to avoid permanent paralysis.
-
Cardiac Emergencies: Myocardial infarctions require immediate thrombolytic therapy or catheterization; every ten-minute delay causes irreversible heart muscle death.
When an industrial site suffers from treatment-delay escalation, an injury that would have resulted in a simple three-week hospital stay in a city turns into a multi-million-dollar fatality or permanent total disability claim. Insurers calculate this mathematical slide toward catastrophic outcomes to adjust their loss reserves.
Stabilization Capability vs. Definitive Treatment Capability
A critical point of confusion for many employers is the difference between having an on-site medic and having a comprehensive medical system. Underwriters separate these into two distinct categories: Stabilization Capability and Definitive Treatment Capability. This distinction forms the backbone of treatment-continuity underwriting.
| Attribute | On-Site Stabilization Capability | Definitive Treatment Capability |
| Personnel | On-site medics, remote paramedics, or nurse practitioners. | Board-certified trauma surgeons, intensive care specialists, and anesthesiologists. |
| Facilities | Rig clinics, containerized first-aid stations, stabilizing bays. | Full-scale hospitals, advanced imaging suites, positive-pressure operating rooms. |
| Interventions | Airway management, temporary splinting, IV access, and temporary trauma stabilization. | Definitive orthopedic surgery, neurosurgery, open-heart interventions, and long-term ICU care. |
| Duration | Designed to sustain life for hours. | Designed for complete recovery and long-term medical stability. |
Underwriters know that temporary stabilization does not guarantee long-term survivability if definitive treatment remains inaccessible for an extended period. For instance, an on-site medic may successfully intubate a worker with a crushed chest injury, but the absence of thoracic surgery options means the patient cannot be cured on-site. Without clear treatment continuity that bridges this gap, the patient will eventually experience post-stabilization deterioration, causing the initial medical stabilization to fail.
Disability Severity Modeling & Catastrophic Amplification
When an injured worker survives an accident but suffers long-term damage, the financial impact shifts to disability lines. Actuaries use disability severity modeling to project the lifetime costs of an injury, and this modeling is directly tied to the speed of early medical intervention.
┌───► Immediate Treatment ───► Full Recovery (Low Claim Cost)
[Trauma Incident] │
└───► Delayed Treatment ───► Catastrophic Disability Amplification (High Claim Cost)
Many remote-work injuries become permanently disabling because delayed stabilization worsens long-term medical outcomes. This is known as catastrophic disability amplification:
-
Neurological Damage Escalation: A spinal or head injury left un-stabilized for twelve hours frequently results in permanent quadriplegia or profound cognitive damage, rather than a partial recovery.
-
Mobility Loss and Spinal Deterioration: Orthopedic fractures that are not properly aligned or tractioned within the early hours can lead to permanent joint destruction, chronic non-union of bones, and a lifelong loss of mobility.
-
Prolonged Oxygen Deprivation: Delayed airway management or lack of high-flow oxygen delivery results in diffuse ischemic brain damage, destroying an individual’s ability to live independently.
-
Delayed Burn Treatment: A failure to initiate specialized skin cooling and advanced fluid management within the first few hours causes partial-thickness burns to convert into full-thickness, third-degree injuries, requiring extensive skin grafting and causing severe permanent contractures.
Specialist-access limitations in remote regions mean that the initial damage becomes permanent before the patient ever sees an orthopedic surgeon, neurologist, or burn specialist, causing an irreversible loss of occupational capacity.
Pricing, Eligibility, and Coverage Restrictions
The economics of underwriting remote risks come down to the severity of potential claims. In accessible areas, insurance claims are balanced across a predictable curve of minor, moderate, and severe outcomes. In remote settings, the middle of that curve disappears; moderate injuries quickly slide into severe or fatal outcomes due to operational medical instability.
This reality increases insurance costs and affects carrier risk appetite across several key dimensions:
-
Severe Disability Exposure: The high probability that a survivable injury will escalate into a lifetime total disability claim requires insurers to hold millions of dollars in active reserves for a single incident.
-
Fatality Escalation: When a remote medical system fails to maintain stabilization, a standard injury claim converts into a high-cost fatality settlement.
-
Evacuation Costs: A single long-range, private air-ambulance or specialized maritime extraction can easily exceed $150,000 to $250,000 per flight depending on geographic isolation, specialized flight crew requirements, and onboard life-support technology. This immediate operational expense is mechanical loss-cost territory borne directly by the policy limits.
-
Prolonged Rehabilitation: Because early treatment delays worsen the initial damage, surviving workers require longer hospital stays, more surgeries, and extensive, long-term rehabilitation.
This increased risk profile creates reserve exposure for the insurance carrier. To protect their financial stability, insurers must charge higher premiums and apply strict deductibles to offset this catastrophic claim severity.
When an insurance carrier determines that an operation’s geographic isolation or environmental risks are too severe, they will pull back their risk appetite. This leads directly to severe coverage restrictions or a complete denial of coverage. Insurers restrict terms based on specific operational vulnerabilities:
-
Extreme Remoteness: Sites located hundreds of miles outside the operational radius of standard medevac aircraft.
-
Weak Rescue Infrastructure: Areas lacking reliable public coast guards, regional trauma networks, or professional search-and-rescue teams.
-
Unstable Medical Systems: On-site clinics that lack proper trauma equipment, medical redundancy systems, or qualified medical personnel.
-
Severe Environmental Exposure: Environments prone to long periods of freezing weather, dense fog, or regular tropical storms that can stop evacuation efforts.
These operational vulnerabilities explain Why Offshore Workers Face Insurance Restrictions in the commercial market. When an underwriter encounters high survivability uncertainty, they will exclude specific types of claims or limit total coverage payouts, forcing the employer to self-insure the remaining exposure.
Complexity & The Contractor Chain
When a serious injury occurs at an isolated job site, the resulting insurance claim is rarely straightforward. Remote medical claims are often operationally complex, leading to extended investigations and detailed reviews by claims adjusters. This complexity stems from several unique operational factors:
-
Delayed Incident Reporting: Due to communication failures or isolated operating conditions, hours or days may pass before the home office or the insurance carrier receives formal notification of an injury.
-
Remote Medical Verification: Adjusters must review medical logs handwritten in a rig clinic or recorded via spotty satellite feeds, making it difficult to establish a clear medical timeline.
-
Contractor Fragmentation: Remote sites often host workers from multiple subcontractors, logistics providers, and third-party agencies, creating confusion over whose policy is primary.
-
Treatment-Documentation Limitations: During a high-stress trauma event with a single medic, detailed chart notes often take a backseat to active life-saving measures, leaving gaps in the formal medical record.
-
Transport-Verification Problems: Tracking the exact timeline of private launch boats, chartered helicopters, and regional ambulances requires extensive logistical auditing.
Geographic jurisdiction also adds complexity. When an incident occurs outside territorial boundaries, adjusters must navigate International Waters Insurance Exclusions to determine how local laws, international maritime conventions, and policy boundaries apply to a delayed stabilization claim.
Contractor Chains & Medical Responsibility Fragmentation
Modern remote operations rarely rely on a single company; they use a complex network of operators, subcontractors, rescue vendors, helicopter providers, offshore medics, and third-party evacuation systems. This interconnected structure can lead to medical responsibility fragmentation.
When an accident occurs, this fragmentation creates liability ambiguity. For example, if a subcontractor’s employee is injured, but the on-site clinic is managed by the primary operator, and the helicopter evacuation is handled by a third-party aviation company, any failure in care becomes difficult to untangle. If the medic runs out of oxygen or the helicopter pilot refuses to fly due to weather, a dispute can break out over which company’s insurance policy must cover the resulting catastrophic disability amplification. Insurers manage this risk by requiring clear indemnity agreements and verifying that all parties across the contractor chain maintain matching medical access standards.
Claims Disputes & Operational Degradation
Because remote medical claims carry significant financial exposure, insurance companies review them with intense underwriting scrutiny. When an emergency evacuation occurs, any deviation from established safety protocols can lead to delayed payments or disputed coverage.
Underwriting Case in Point: Consider an oil and gas subcontractor operating in the Gulf of Mexico that deployed an unvetted offshore supply vessel to evacuate a worker with a severe crush injury after bad weather grounded local aviation. Because the vessel lacked a marine medical certification and lacked basic stabilization equipment, the worker suffered severe post-stabilization deterioration during the transit. The resulting catastrophic disability claim became the subject of an extended coverage dispute involving alleged breaches of declared evacuation procedures.
The most frequent claim disputes stem from clear operational violations:
-
Unauthorized Evacuation Methods: Utilizing a non-medically certified supply boat or a local commercial helicopter that lacks proper life-support equipment to transport a critical patient.
-
Unapproved Transport Providers: Contracting a rescue flight with a local aviation firm that has not been vetted or approved by the insurer’s risk-control team.
-
Undeclared Remote Assignments: Deploying personnel to an isolated exploration zone or offshore sector without notifying the underwriter or adding the location to the policy roster.
-
Expired Emergency Certifications: Allowing on-site medics or rescue teams to operate with lapsed advanced cardiac life support (ACLS) or trauma certifications.
-
Inaccurate Occupational Disclosures: Classifying a worker as an onshore administrative employee when their actual duties involve traveling to remote, unstable offshore platforms.
-
Failure to Follow Evacuation Procedures: Initiating a complex rescue without contacting the designated medical advisory hotline required by the policy.
Underwriting Breakpoint: If an employer’s declared evacuation procedures differ materially from the systems actually used during an emergency response, insurers may argue that the operational risk presented at the claim stage no longer matches the original underwriting assumptions. If an operator fails to follow their declared emergency response plan, they run the risk of breaking policy warranties, which can lead to denied claims and full exposure to the loss.
Environmental, Logistical, and Human Degradation
The structural failure paths of remote operations can be categorized across three distinct operating vectors:
| Operational Failure Vector | Primary Medical Trigger | Underwriting Consequence |
| Medevac Dependency | Helicopter systems vulnerable to fog, ice, and weather grounding; transport instability degrades patient during transit. | Increased catastrophic severity exposure; mandatory analysis of Helicopter Transport Risk in Offshore Insurance and Offshore Evacuation Risk and Insurance. |
| Environmental Severity | Storms ground aircraft; cold exposure accelerates trauma-induced coagulopathy; waves disrupt delicate subsea/on-site intubations. | Interruption of treatment continuity; acceleration of internal bleeding; escalation of reserve requirements. |
| Worker Fatigue & Isolation | 12-hour shifts and extended hitches cause cognitive deterioration; medics make tracking errors; team leaders face decision degradation. | Higher risk of misdiagnosis; structural reliance on Offshore Rotation Work and Disability Insurance frameworks to evaluate risk. |
| Medical Capacity Saturation | Multi-casualty industrial disasters overwhelm lone remote medics, causing rapid triage degradation and equipment shortages. | Evacuation overload; complete collapse of individual survival windows; severe multi-casualty reserve exposure. |
| Operational Remoteness | Physical infrastructure layout (e.g., turbine height, mine shafts) introduces heavy rescue degradation before clinic arrival. | Loss of the structural “Golden Hour”; inflation of projected injury severity over a twelve-to-forty-eight-hour un-stabilized window. |
| Medical Capability Degradation | Extended isolation drains limited trauma equipment, medication volumes, oxygen supply, and satellite telemetry links. | Post-stabilization deterioration; complete failure of initial stabilization; misalignment with OSHA emergency guidance. |
How Employers Improve Operational Insurability
Employers can secure better insurance rates and protect their access to coverage by improving their on-site survivability preparedness. Underwriters look for proactive investments that demonstrate true operational medical resilience. Ultimately, employers improve operational insurability by reducing survivability uncertainty. To build a strong underwriting profile, companies should focus on several key areas:
-
Emergency-Response Planning: Developing detailed, audited medical protocols that outline every stage of an emergency response, from initial injury to final hospital drop-off.
-
Trauma-Preparedness Systems: Equipping on-site clinics with advanced life support gear, such as ventilators, automated external defibrillators, and advanced airway management tools.
-
Medevac Partnerships: Securing priority-service contracts with licensed, medically certified aviation and marine evacuation providers.
-
Communication Redundancy: Deploying multiple, independent communication systems, such as satellite phones, cellular boosters, and dual-network radios, to ensure constant contact with medical control.
-
Stabilization Equipment: Stocking specialized medical kits, blood products, and advanced medications to manage severe trauma for extended periods.
-
Fatigue Management: Implementing clear shift-length limits, mandatory rest periods, and health monitoring programs to prevent worker and medic exhaustion.
-
Rescue Drills: Conducting regular, unannounced emergency drills with on-site workers and external rescue teams to test response times and communication links.
-
Environmental Monitoring: Using real-time weather tracking and forecasting tools to anticipate storm fronts or visibility drops that could interrupt evacuation routes.
-
Medical Redundancy Systems: Maintaining backup power grids, independent oxygen concentrators, and cross-trained first responders to prevent a single point of failure from disabling the clinic.
When an underwriter sees these safety measures in place, their confidence in the site’s stabilization probability increases, which helps secure competitive premium rates and broader policy terms.
Real-World Remote Medical Underwriting Examples
To see how these concepts apply in real life, consider how underwriters analyze these realistic remote-work scenarios:
Scenario 1: Delayed Offshore Cardiac Evacuation
An offshore worker on a vessel experiences an acute myocardial infarction during a storm. The vessel lacks a thrombolytic medical kit, and a helicopter cannot land due to high winds. The evacuation delay stretches to fourteen hours, resulting in severe, permanent cardiac muscle death and irreversible congestive heart failure.
-
The Insurance Consequence: The claim escalates from a standard medical event into a lifelong total disability payout due to the lack of on-site stabilization capabilities and weather-driven evacuation delays.
Scenario 2: Remote Burn Stabilization Failure
An explosion at an isolated mining operation leaves a technician with deep partial-thickness burns across 40% of their body. The on-site clinic has an inadequate supply of sterile saline and lacks advanced fluid-resuscitation protocols. During a twelve-hour overland ambulance transport, the worker enters severe hypovolemic shock, causing acute kidney failure.
-
The Insurance Consequence: The underwriter must cover a multi-million-dollar catastrophic claim for long-term dialysis and extensive skin reconstruction, driven by the site’s failure to maintain operational medical resilience.
-
Underwriting Impact: Following severe claims like this, insurers frequently reevaluate whether the operation’s medical redundancy systems and evacuation partnerships remain acceptable for continued coverage eligibility.
Scenario 3: Wilderness Pipeline Rescue Breakdown
A heavy equipment operator on a wilderness pipeline project suffers a severe crush injury to their leg, resulting in a fractured femur and an arterial bleed. The crew’s satellite phone fails, delaying the emergency call by three hours. By the time a rescue team arrives, prolonged blood loss has caused severe hypoxic brain injury.
-
The Insurance Consequence: A standard orthopedic injury converts into a permanent, high-cost cognitive disability claim, highlighting how communication failures directly worsen injury outcomes.
Key Takeaways
-
Underwriting Focus: Remote medical access insurance assesses an operation’s ability to keep an injured worker stable during an extended rescue window, rather than simply tracking how often accidents occur.
-
The Cost of Delay: Golden Hour degradation and treatment delays cause standard injuries to escalate into permanent disabilities or fatalities, driving up insurance costs.
-
Evacuation Realities: Relying on a basic medevac plan is not enough; underwriters calculate real-world evacuation survivability based on weather vulnerabilities, transport stability, and system redundancies.
-
System Integrity: Insurers look closely at medical redundancy systems and operational medical resilience to ensure an on-site clinic can handle extended care and multi-casualty events without failing.
- Disability Outcomes: Specialist-access limitations in remote areas accelerate long-term disability claims, making early, on-site stabilization critical for keeping insurance costs manageable.
Final Underwriting Insight
In remote medical access insurance, insurers are not only evaluating whether workers may become injured; they are evaluating whether operational medical systems can realistically preserve survivability long enough for advanced treatment to remain achievable under delayed-response conditions.
True operational survivability requires a clear understanding of stabilization probability and treatment continuity. By managing medevac dependency and building resilient medical redundancy systems, employers can protect their workforce from Golden Hour degradation and post-stabilization deterioration, transforming an uninsurable risk into a well-managed, insurable operation. In many remote operations, the true underwriting risk is not the injury itself, but whether the operational environment allows survivability to remain medically sustainable long enough for advanced intervention to occur.
—————————————————————————————————————————
Institutional & Underwriting Reference
-
Occupational Safety and Health Administration (OSHA) – Emergency Preparedness & Response
Referenced for emergency-response systems, delayed rescue exposure, remote industrial incident management, and operational safety standards affecting survivability underwriting.
-
National Institute for Occupational Safety and Health (NIOSH)
Referenced for occupational fatality exposure, remote worker safety research, industrial trauma risk, and environmental operational hazards.
-
World Health Organization (WHO) – Emergency Care Systems
Referenced for trauma-system stabilization frameworks, treatment-delay severity, emergency survivability systems, and advanced-care accessibility.
-
International Maritime Organization (IMO) – Search and Rescue Standards
Referenced for offshore rescue coordination systems, maritime evacuation procedures, delayed extraction risk, and survivability continuity frameworks.
-
National Oceanic and Atmospheric Administration (NOAA) – Weather & Marine Forecasting
Referenced for offshore weather disruption exposure, evacuation instability, storm-related rescue delays, and environmental survivability deterioration.
-
International SOS
Referenced for remote medical logistics, evacuation dependency systems, international medevac coordination, and operational medical resilience.
-
Society of Petroleum Engineers (SPE)
Referenced for offshore operational systems, energy-sector emergency preparedness, remote workforce logistics, and medical redundancy planning.
Reviewed for Underwriting Accuracy
This article was reviewed for underwriting accuracy using operational and occupational survivability analysis relevant to:
-
Remote medical access insurance
-
Offshore evacuation underwriting
-
Treatment-delay severity modeling
-
Operational survivability analysis
-
Medevac dependency exposure
-
Golden Hour degradation underwriting
-
Catastrophic disability amplification
-
Remote trauma stabilization systems
-
Specialist-access limitations
-
Rescue-delay severity modeling
-
Environmental evacuation instability
-
Operational medical resilience frameworks
-
Offshore and remote workforce underwriting
-
Multi-casualty medical saturation exposure
-
Treatment continuity and post-stabilization deterioration